
A cavitation is a hole in the bone, often where a tooth has been removed and the bone has not filled in properly. In the last several years, the term cavitation has been used to describe various bone lesions which appear both as empty holes in the jawbones and holes filled with dead bone and bone marrow(5). Dead, cavitational areas, which produce pain, are now called NICO (Neuralgia Inducing Osteonecrosis) lesions(6). Cavitations are often a result of either ischemic osteonecrosis, due to poor blood flow in the marrow, or a traumatic bone cyst. In his book on oral pathology, Dr. G.V. Black, one of the early experts on cavitations, suggested surgical removal of these dead bone areas. Other less traumatic measures are now first used and surgery with curetting is used primarily where the patient has significant health effects not resolved by other means. When a tooth is being extracted, in what has been normal dental procedure, the surrounding periodontal membrane is usually left behind. Theoretically, when a tooth has been pulled, the body will eventually fill in the space in the bone where the tooth once was. But when the membrane is left behind, an incomplete healing commonly takes place which leaves a hole or a spongy place inside the jaw bone. Experts speculate that perhaps this is because the bone cells on either side sense the presence of the periodontal membrane and “think” that the tooth is still there. This appears to be one common cause of cavitations. (1,3-5,16-22,29-32,45)
Endodontic cysts are also commonly occurring usually in the gums at the tip of a tooth, that have pockets of bacterial infection that can cause inflammation and pain in some cases similar to cavitations (48,49,33). Bacterial infections are also known to have systemic effects.
A cavitation can form in any bone in the body, not just in the jaw bones. There are also other reasons that cavitations form, some of which are localized traumas, poor circulation to the area, clotting disorders, and the use of steroids.
On X-ray of an extracted tooth site, this membrane can form an image that appears to be a shadow of a tooth. Almost always, this is indicative of a cavitation. Most dentists are aware of this phantom tooth image, but they do not recognize it as a site of potential problems. Other means of locating or identifying cavitational areas include sonic imaging(CAVITAT)(3,68), local anesthesia, Spect Scan(65), pressure to determine trigger points, Computer Electro Dermal System(67), etc. While positive Spect Scans were found in 19 of 20 patients with jaw pain, several control patients with no pain also had positive scans- often finding previous jaw pathoses. Thus the Spect Scan was not sensitive at differentiating painful from non-painful conditions. Some of the other methods had more success at such differentiation.
What’s hiding inside?
Inside a cavitation, bacteria flourish and deviant cells multiply. Cavitations act as a breeding ground for bacteria and their toxins. Research has shown these bacterial waste products to be extremely potent(7,8). Cavitations can also cause blockages on the body’s energy meridians and can exert far-reaching impact on the overall system. Investigation has revealed that some cavitations are reservoirs of huge amounts of mercury and other toxic substances. Cavitations may be a source of low level or high level stress on the entire body. (1-73)
How toxic are cavitations and what type of effects are caused by cavitations?
The results of recent research of Dr. Boyd Haley (former Chairman, Department of Chemistry, University of Kentucky) show that ALL cavitation tissue samples he’s tested contain toxins, which significantly inhibit one or more of the five basic body enzyme systems necessary in the production of energy(7,8). These toxins, which are most commonly likely to be metabolic waste products of anaerobic bacteria (bacteria which don’t live in oxygen), may produce significant systemic effects, as well as play an important role in localized disease processes, which negatively affect the blood supply in the jawbone.
There are indications that other types of toxins also accumulate in cavitations, and when these toxins combine with certain chemicals or heavy metals (for example, mercury), much more potent toxins may form(5-15).
High levels of mercury are commonly found in some cavitations and in general in the jawbone of those with mercury amalgam fillings and to have significant local and systemic effects (79). Mercury is known to be extremely toxic and to commonly cause chronic adverse local and systemic health effects (70). Yeast and fungi have also been found to accumulate in cavitations, and to have significant systemic effects (10-14).
Accurate tests for cavitation related bacterial toxins have been developed by the Affinity Laboratory in Kentucky, based on research by Chemists from the Univ. of Kentucky Dept. of Chemistry (7,8). The toxins released by anaerobic bacteria in cavitations have been found to be extremely toxic, and to have major effects on necessary body enzymes and the immune system.
Cavitations are Very Common
One study(1,20) of cavitation incidence involved an analysis of 112 randomly selected dental patient charts who had been tested for cavitations, with patient age ranging from 19 to 83 years among 40 males and 72 females. The cavitations were tested for using exploratory drilling. Cavitations were found at approximately 75% of all extraction sites examined.
The most commonly extracted teeth, the third molars (“wisdom teeth”), produced CVs that were found by clinical exploration in 313 out of 354 extraction sites (88%). Cavitations were found in 35 of 50 second molar extraction sites (70%), and for first molars, 60 of 73 extraction sites showed CVs (82%). They were found in 441 of the total number of 517 molar extraction sites explored (85%). For the maxillary non-molars, CVs were found in 72 of 123 extraction sites (58%), and for mandibular non-molars, 23 of 51 extraction sites were affected (45%). For all non-molars, the CV rate was 55%, representing 95 of 174 extraction sites. Note that the cavitations found were not all related to pain or known chronic conditions, and dental patients who had been tested for cavitations is not the same as the general population, so the general population likely has a somewhat lower cavitation incidence.
Bob Jones is the inventor of the CAVITAT -an ultrasound instrument designed to detect and image cavitations that has been approved for testing for cavitations by the FDA after undergoing FDA clinical trials (2b). He found cavitations of various sizes and severity in approximately 94% of several thousand wisdom teeth sites scanned(2a). He also found cavitations under or located near over 90% of root canal teeth scanned in both males and females of various ages from several different geographic areas of the United States. Note again that the population being tested for cavitations in these trials is not the same as the general population, which might have a somewhat lower incidence of cavitations. But its clear that the occurrence is very common.
Confirmation of cavitation necrosis and toxicity is commonly by 2 or the leading labs in the U.S. with technology for performing such tests, the Maxifillial Center in West Virginia and the Affinity Laboratory in Kentucky.(5-8). Analysis typically finds clear evidence of chronic intraosseous inflammation- often with dense marrow fibroisis or nonresorbing necrotic bone flakes with very little healing or new bond formation(6). It has also been found that these lesions often spread to other areas to initiate further cavities.
Root Canals and Cavitations
Research has demonstrated that virtually all root canals result in residual infection due to the imperfect seal that allows bacteria to penetrate. The most commonly used material in root canals is gutta percha, which is soaked with chloroform and heated. But when the chloroform evaporates and the gutta percha cools, there is significant shrinkage in all such root canal fillings, which allows entrance of bacteria(18-22,50). A condition that commonly occurs with root-canaled teeth is a radicular or periapical cyst or apical periodontis, which is a pocket of bacterial inflammation that often forms in the gums at the tip of root-canaled teeth(48,49,52,53) due to bacteria inhabiting the tooth. These are the most common type of cysts that form in the gums and can also be a factor in formation of cavitations in the neighboring jawbone. Once established, nonmutans streptococci, enterococci and lactobacilli appear to survive commonly following endodontic root-canal treatment of teeth with clinical and radiographical signs of apical periodontitis (51). Large scale tests found cavitations under or located near approx. 90% of root canal teeth scanned in both males and females of various ages from several different geographic areas of the United States(2). The general population could be somewhat different from this sample as the sample was not a random sample. In tests of 745 randomly chosen root-canaled teeth at a dental school, done at least 1 year prior to test, 33% were found to have apical periodontitis(53).
The toxins given off by these bacteria are often even more toxic than mercury(7-10). The bacterial toxins from root-canaled teeth and associated cavitations can cause systemic diseases of the heart, kidney, uterus, immune, nervous and endocrine systems.
A useful and commonly used test to assess the cause of toxic related chronic health conditions is the urinary fractionated porphyrin test, which measures the degree that toxic exposures have blocked digestive enzymatic processes necessary to the function of the body, by looking at the level of various waste porphyrins in the urine caused by these blockages. The level of such toxic related porphyrins in the urine of people with chronic conditions including Parkinson’s have been found to decline in some patients after cavitation treatment(or amalgam removal). (20). This is also been found for many cases of Lupus and MS(78,38). Lupus symptoms are often associated with blockage and resulting high levels in urine of Uriporphyrin, while MS is more commonly associated with high Coproporphyrin.
Cavitation Treatment usually results in significant pain improvement
Cavitations commonly cause adverse health effects, and many thousands of cavitations have been treated. They are commonly tested or biopsed by labs having the expertise to provide these services, and virtually all that have been tested or biopsed were found to be associated with dead, necrotic tissue and extreme toxicity(3,5-9). The types of conditions that cavitations have been most commonly related to are atypical facial neuralgia, trigeminal neuralgia, chronic sinusitis, phantom toothache pain, and headaches including migraines.
Dr. Briener, DDS, and others recommend two primary methods of treatment for their patients(40,54,33,etc.). First is a procedure where special homeopathic medications called Sanum remedies are injected into the cavitation site, and then a modified form of infrared light or low level laser light therapy is applied to the area. In some cases the light therapy alone has been sufficient to resolve the problem(54). This is often successful in cases related to smaller cavitations with primarily poor blood flow or bacterial toxin effects. Cavitations have also been treated successfully using oxygen/ozone therapy(74). Although cavitations are very common, they should only be treated surgically if there is indication of a relation to pain or chronic health effects not resolved by other means. There are various ways to assess this.
If this method is not successful, the alternative is to surgically open the area and clean the remaining ligament and resultant debris from the bone. Every biopsy of bone material he has collected from cavitation surgeries has shown osteonecrosis, or dead bone material. In all studies reviewed, the majority of those undergoing surgery for NICO pain had significant pain relief after surgery(3-Table1,40,42-45,55-
French and German oral surgeons have developed an alternative method of minimally invasive cavitation surgery (41).
Due to the nature of the mechanisms related to cavitation formation, it is not uncommon for cavitation sites that are treated to become reinfected or to accumulate other toxins that can cause a relapse of symptoms. Such cases may require retreatment using either surgery or other options.
Chronic health conditions other than pain related to cavitations and oral bacteria levels
Many researchers today believe that NICO lesions, like periodontal disease, is the focus of various infections which may spread throughout the body and have systemic effects. In the last few years, some of the most surprising medical news has been the discovery that bacteria from the mouth appear to be very influential in causing various heart, liver, kidney, and immune problems(68).
Researchers from New York University found that certain bacteria from the mouth may be related to preterm delivery and low birth weight according to a study in the Journal of Periodontology (JOP). (68b) The presence of specific bacteria and combinations of bacteria in periodontal pockets also appears to be responsible for the relationship between periodontal disease and acute coronary syndrome (ACS), according to a new study published in the Journal of Periodontology (68c).
Dr. Weston Price was a prominent dental researcher leading a medical research team on the relation between root-canal teeth and chronic health conditions(70). Through a long series of well documented clinical cases and experiments his team found that root-canals accumulate bacteria that give off extreme toxins sufficient to cause serious health conditions, including cancer(22,25,28,29,36,37, 38,46,47,70,etc.) , cardiovascular conditions(19-22,29,36,38,70,
Many doctors and dentists through their experience with patients have reached similar conclusions (18-26,28,29,32-39,45,54-65,
Modern experiences also support this theory. Dr. Issels, a German physician, recommends extraction of root canal teeth as part of his protocol for terminal cancer patients. Over the last 40 years with 16,000 patients, he has observed a 24% total remission rate(46,25).
Dr. Florian Kubitzek, a physician and dentist in Munich, Germany, uses the CT scan to study the teeth and jaw. His scanning technique has been invaluable in diagnosing jaw abscesses below the teeth that have been inadequately treated by standard dentistry. Conventional dental X-rays have entirely missed the jaw abscesses known as cavitations. Kubitzek treats many cancer patients who have dental cavitations as a collaborative approach in the overall treatment of metastatic and primary cancer(37).
Dr. John Diamond(MD) says that all patients with breast cancer that he has tested had root canals on the tooth related to the breast area on the associated energy meridian.” (25)
Other clinics that treat cancer have similarly found that most of their patients with cancer have root-canaled teeth or cavitations and that treating these is an important part in success at treating cancer(38,39)
Research and clinical cases have found cavitations to be related to many chronic health conditions which have improved after cavitation treatment, including cancer, congestive heart failure and other cardiovascular problems, lupus, rheumatoid arthritis, and autoimmune conditions- perhaps related to cavitations major effects on the immune system.
If you have a joint implant or mitral valve prolapse, your dentist must prescribe an antibiotic before any dental treatment. Why? Because bacteria from the mouth can spread through the blood to cause serious problems elsewhere in the body. There is growing evidence that the toxins from NICO lesions do the same.
Trigeminal Neuralgia, one of the most severe painful conditions which occurs to man and women , many other face and jaw neuralgic illnesses, have for the most part, had unknown causes until recently. The discovery of paw bone infections ( cavitations lesion ) is proving an important reason for the occurrence of high percentage of these diseases. Their correction has achieved an impressive cure rate. In view of the subject matter of the Root Canal Cover- up , the fact of Root filled teeth being cause of these cavitations infections should be if particular interest
J.E. Bouquot, D.D.S. , M.S.D.
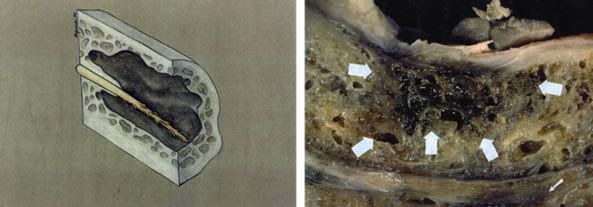
Photo from J.E. Bouquot D.D.S figure top drawing of atypical cavitating NICO lesion of the mandible shows an irregular outline, darkened walls, destruction of the inferior alveolar canal, and a frayed rope appearance to the exposed neurovascular bundle. Figure bottom. A large NICO lesions is seem in the mandibular molar region ( large arrows ) . The small arrows point to a less severely involved second site of ostonecrosis just above the inferior border and involving the inferior alveolar nerve.
A cavitation refers to a toxin-containing hole in the jawbone, often at the site of a previously extracted tooth. Cavitations have many scientific names such as ischemic osteonecrosis, chronic non-superative osteomyelitis, and neuralgia inducing cavitational osteonecrosis (NICO). This is not so much an infection in the bone, as a necrosis or gangrene (dead tissue) in the bone marrow, as a result of impaired blood flow (ischemia). A cavitation often develops because of incomplete healing after routine extraction. The contents of cavitations are always necrotic, dead or dying material. The microscopic picture looks the same as gangrene! If a gangrenous extremity is not amputated, the rest of the body will sicken and die, due to a high concentration of anaerobic bacterial toxins.
Incomplete healing of a cavitation is promoted by a number of factors, including the following:
- Failure to completely remove the periodontal ligament lining the tooth socket that holds the tooth to the bone
- Physically large surgical excavations, such as with impacted wisdom teeth, where the resulting holes can be expected to be larger than usual and more new bone is required to fill the holes
- Failure to clean out the infected adjacent bone and periodontal ligaments seen in the extraction of root canal treated and abscessed teeth
- Failure to remove condensing osteitis, the reactive bone formation that attempts to wall off infection, usually involving the periodontal ligament as well
- Poor systemic healing support from a compromised immune system
- Poor nutrition and a weak thyroid gland.
- Failure to allow the formation of a complete blood clot at the excavation site; too early dislodgment of a clot after extraction; also bleeding
- Smoking
- Antibiotic therapy
- Chronic osteoporosis of the jawbone
- Systemic and adjacent toxicity from other dental toxins and other sources
- Pre-existing periodontal disease, in addition to any other factor that would also promote periodontal disease
One of the primary factors in cavitation formation seems to be that the initial extraction does not include the thorough removal of the periodontal ligament from the socket after the tooth is removed. Unfortunately, this inadequate socket cleaning is the routine procedure with most extractions. Cavitation formation after tooth extraction is the rule and not the exception; yet, the condition is still largely unknown to most of dentistry, and underestimated by those who are aware of it. A cavitation can be expected to form when the socket lining separating the tooth from the bone is not thoroughly removed. A thorough removal of the ligament requires that a portion of the bony socket be removed as well.




